Urine Diagnostics in Hyponatremia

Check out the The Hyponatremia Menu for a general approach to differential diagnosis and therapy of hypotonic hyponatremia.
Hypotonic hyponatremia results from four basic pathogenic mechanisms:
High free water intake
High ADH
Diluting defect
Low non-electrolyte solute excretion
When treating patients with hyponatremia, the presence and extent of all four of these mechanisms have to be checked concurrently.
The Spot Urine panel of hyponatremia
This is most easily done by determining the
free water excretion rate,
urine osmolality and
urea excretion rate
from a spot urine analysis of sodium, potassium, urea, creatinine and osmolality:
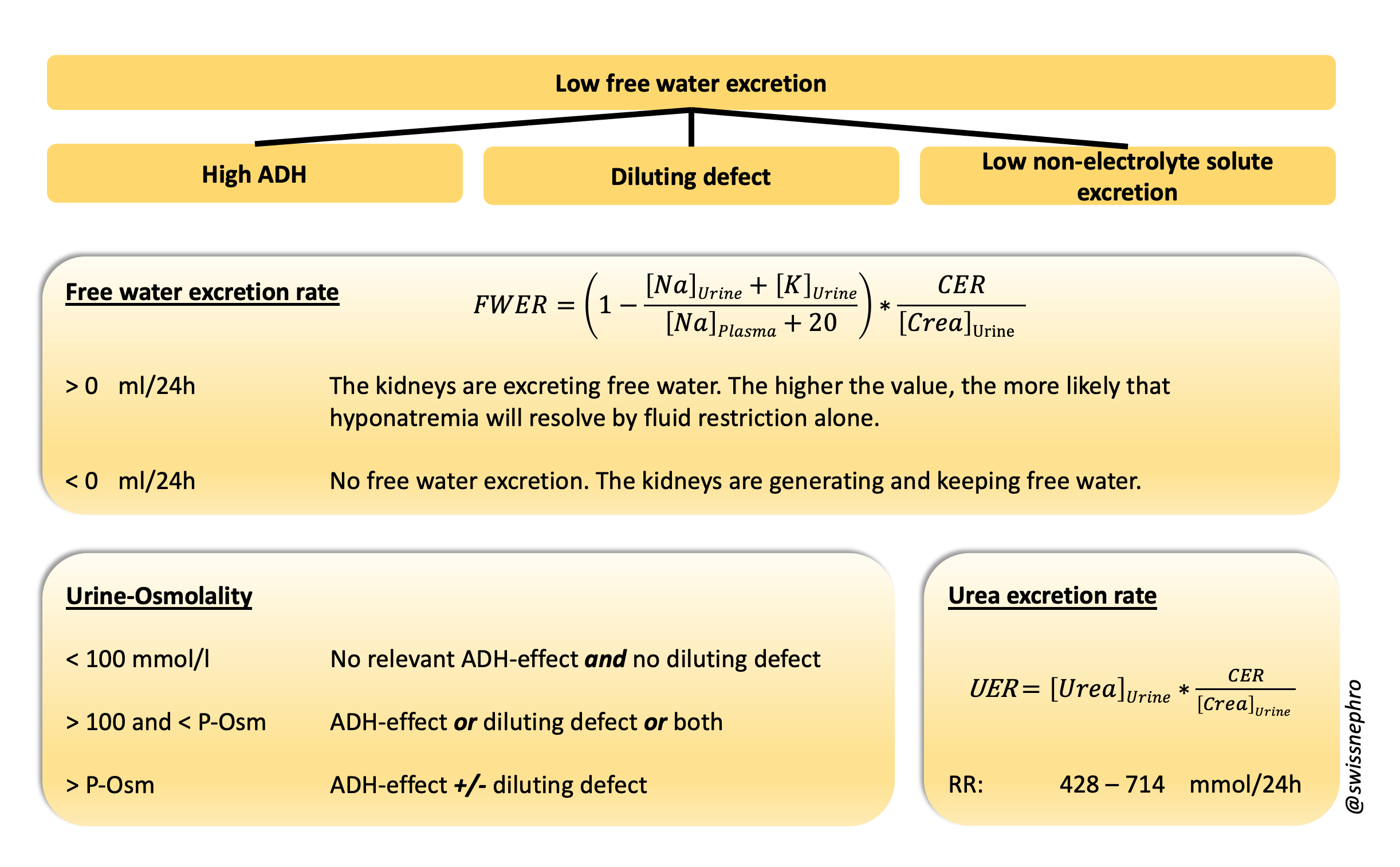
Urine Tests of Hyponatremia: Free water excretion rate (FWER), urine osmolality and urea excretion rate (UER) and their relationship to the general mechanisms of low free water excretion. Note, that all three tests give quantitatively continuous results.
CER creatinine excretion rate, P-Osm plasma osmolality, RR reference range
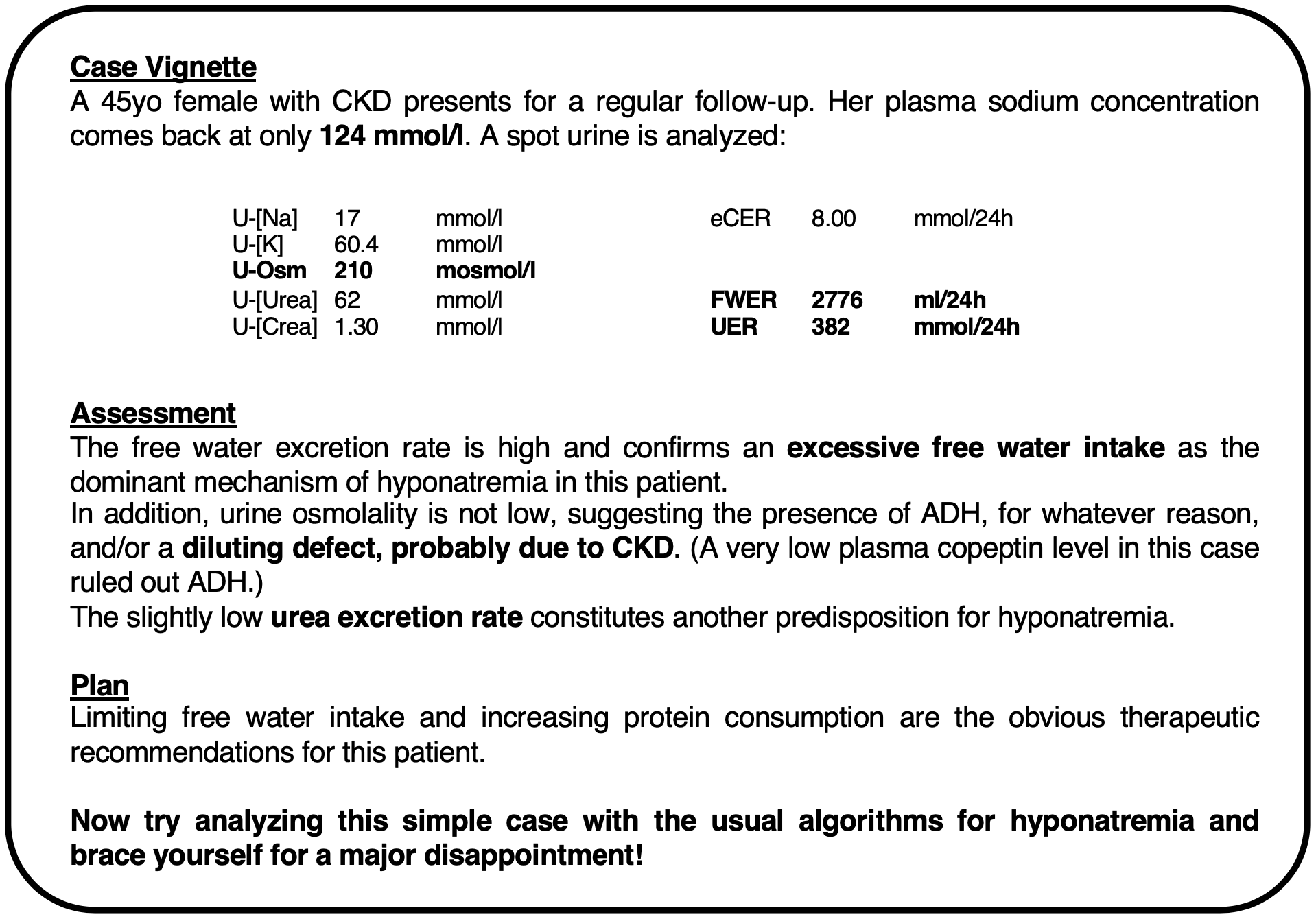
An example of how to apply these tests in clinical practice is presented in the insert.
Comments:
The Free Water Excretion Rate (FWER), also called the “electrolyte free water clearance“, gives a continuous measure of the total free water excreted by the kidneys. It is a fast, global test of the adequacy of the kidneys’ response to hyponatremia. In patients with stable plasma sodium concentrations, FWERs can be used as an indirect measure of free water intake.
Urine osmolality is the most straightforward way to check for the presence and magnitude of ADH and a diluting defect.

The sum of the urine sodium and potassium concentrations can be used as a reasonably good substitute:
Further assessment of the etiology of high ADH and a possible diluting defect, usually requires a comprehensive medical evaluation. Singular tests like the urine sodium concentration and/or clinical volume assessment do not suffice here, as the different categories and multiple causes of high ADH and diluting defects are often simultaneously present in the very same patient.
Non-electrolyte solute excretion is oftentimes neglected as an etiological factor in hyponatremia, although it is a very important quantitative determinant of free water excretion and a common therapeutic target. It mostly depends on dietary protein intake and is best assessed by calculating the urea excretion rate and comparing it to reference ranges and urine osmolality.
In the era of SGLT2-inhibition, glucosuria commonly contributes to non-electrolyte solute excretion. Since it increases free water excretion, glucosuria does not cause hyponatremia and can be ignored here.
All urine tests of hyponatremia only represent the situation at the time when the sample was taken, and do not necessarily reflect the reasons why hyponatremia developed in the first place.
Calculating free water and urea excretion rates from spot urine samples requires an estimate of creatinine excretion. Using current US reference data, I recommend 10mmol/24h for females and 15mmol/24h for males as a starting point.
All necessary calculations can easily be done in the head. If you are reluctant to do so, you can use the following calculator:
Bottom line
Check free water excretion rate, urine osmolality and urea excretion rate for differential diagnosis and therapy of hyponatremia.